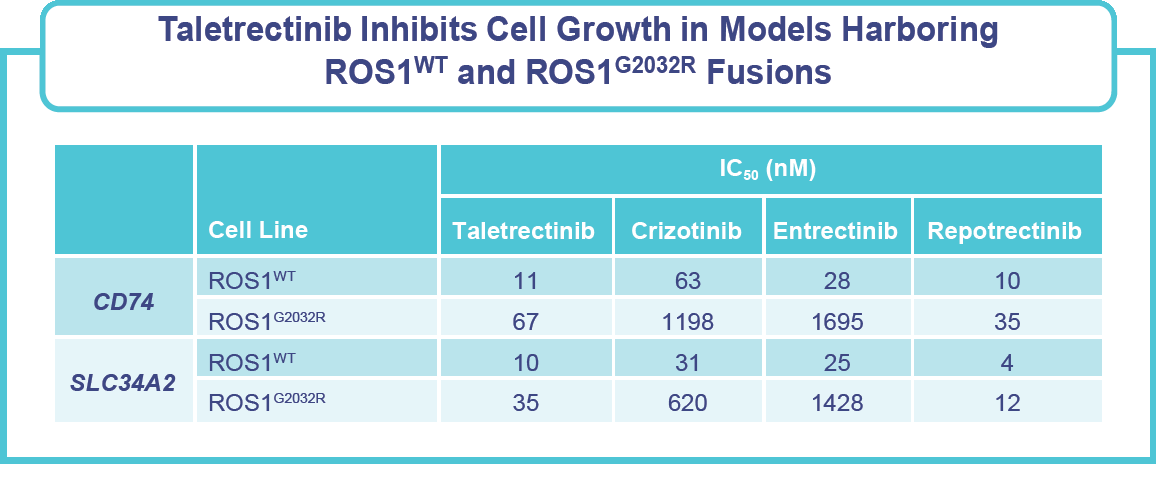
- ROS1 fusions are present in approximately 2% of patients with non–small cell lung cancer (NSCLC), driving cancer cell growth and survival.1
- FDA-approved tyrosine kinase inhibitors (TKIs) for ROS1 fusion-positive NSCLC include crizotinib, entrectinib, repotrectinib and more recently, taletrectinib.1
- Taletrectinib is a potent, CNS-active, selective, next-generation ROS1 TKI for the treatment of patients with locally advanced or metastatic ROS1-positive NSCLC.
- Taletrectinib is currently approved by the FDA and is also approved in China and Japan; additionally, the EMA validated the Marketing Authorization Application for taletrectinib in Europe.
- Among patients with advanced ROS1-positive NSCLC as of August 31, 2025, pooled results from the TRUST-I and TRUST-II studies of taletrectinib demonstrated2:
- TKI-naïve: a confirmed objective response rate (cORR) of 89.8%, an intracranial cORR of 76.5%, a median duration of response (mDOR) of 49.7 months, and a median progression-free survival (mPFS) of 46.1 months.
- TKI-pretreated: Durable responses were also reported in patients who had previously received a TKI.
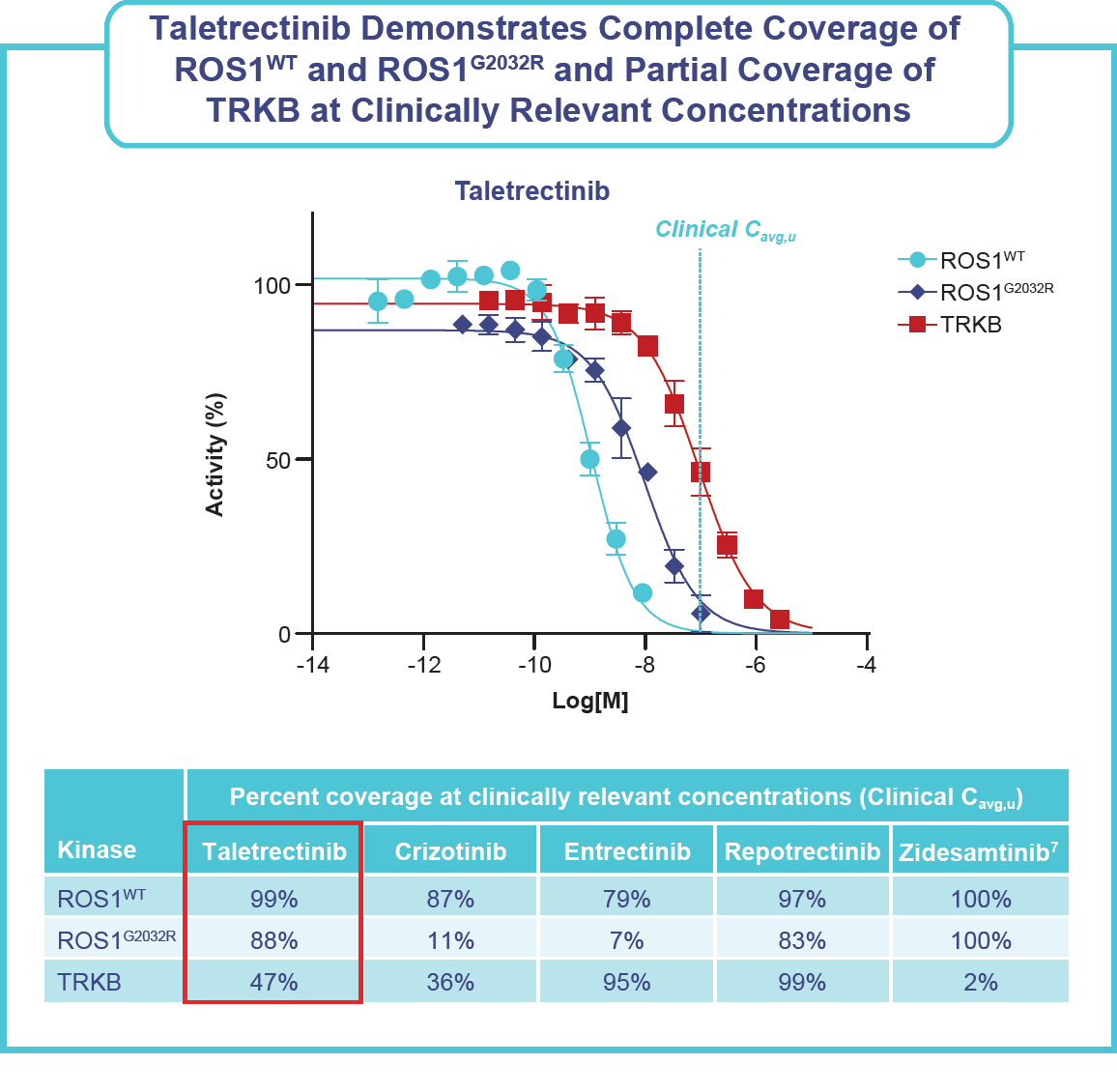
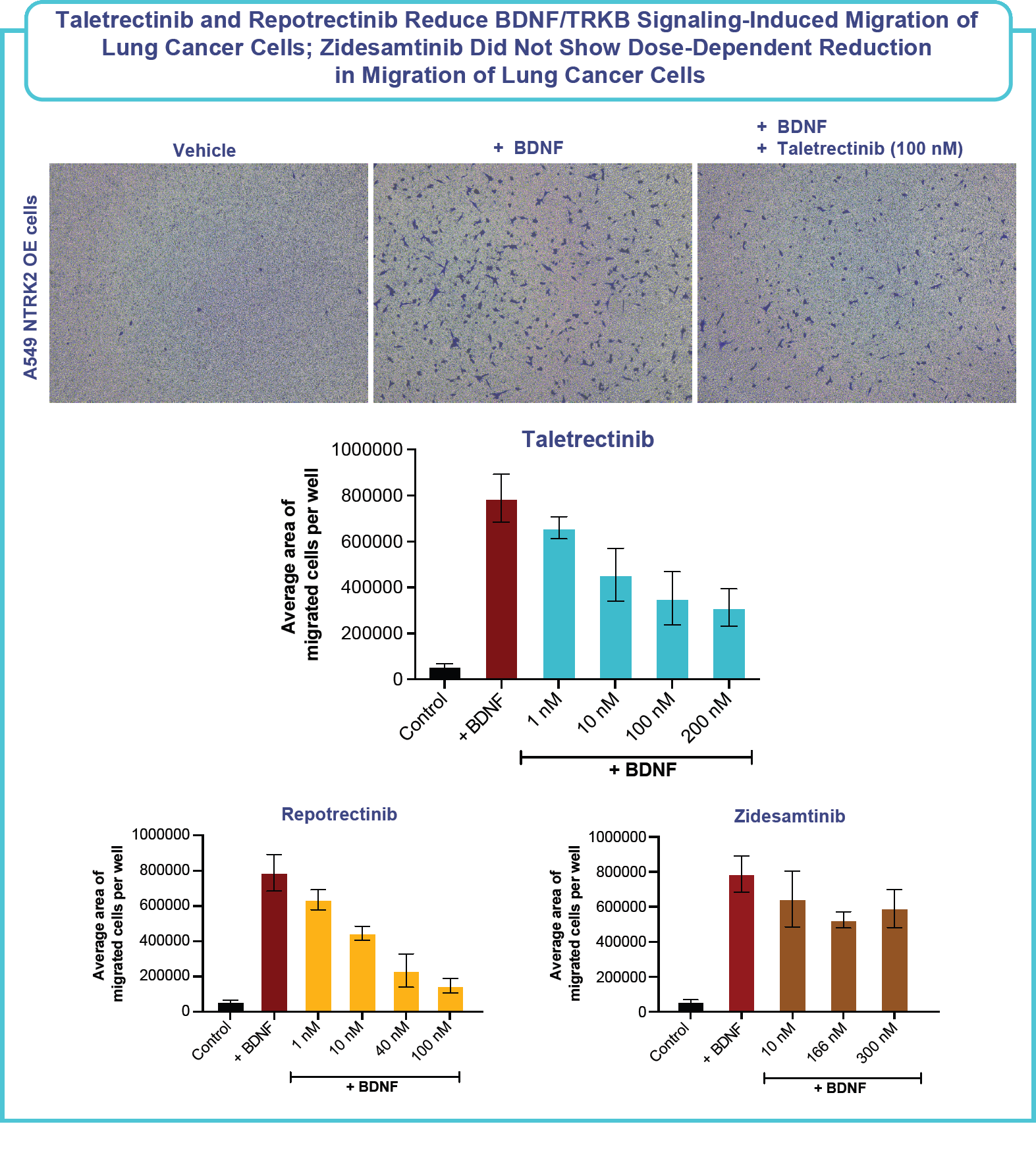
- Despite inhibitory effects of taletrectinib on the tropomyosin receptor kinase B (TRKB), neurologic treatment emergent adverse events (TEAEs)* were infrequent (dizziness, 21%; dysgeusia, 15%) and mostly grade 1.
*The integrated safety population includes TKI-naïve and TKI-pretreated patients with ROS1+ NSCLC who received ≥1 dose(s) of taletrectinib 600 mg QD from Phase 2 trials (TRUST-I and TRUST-II) and a Phase 1 trial (J102)
- Several potent TRKB inhibitors, including repotrectinib, entrectinib, and larotrectinib, are associated with significant rates of neurological adverse events (AEs).
- Neurologic AEs related to TRKB inhibitors, such as cognitive impairment, dizziness, ataxia, and peripheral neuropathy, are undesirable; however, a recent publication by Camidge et al hypothesizes that the potential benefit of CNS protection from TRKB inhibition may outweigh these AEs.3
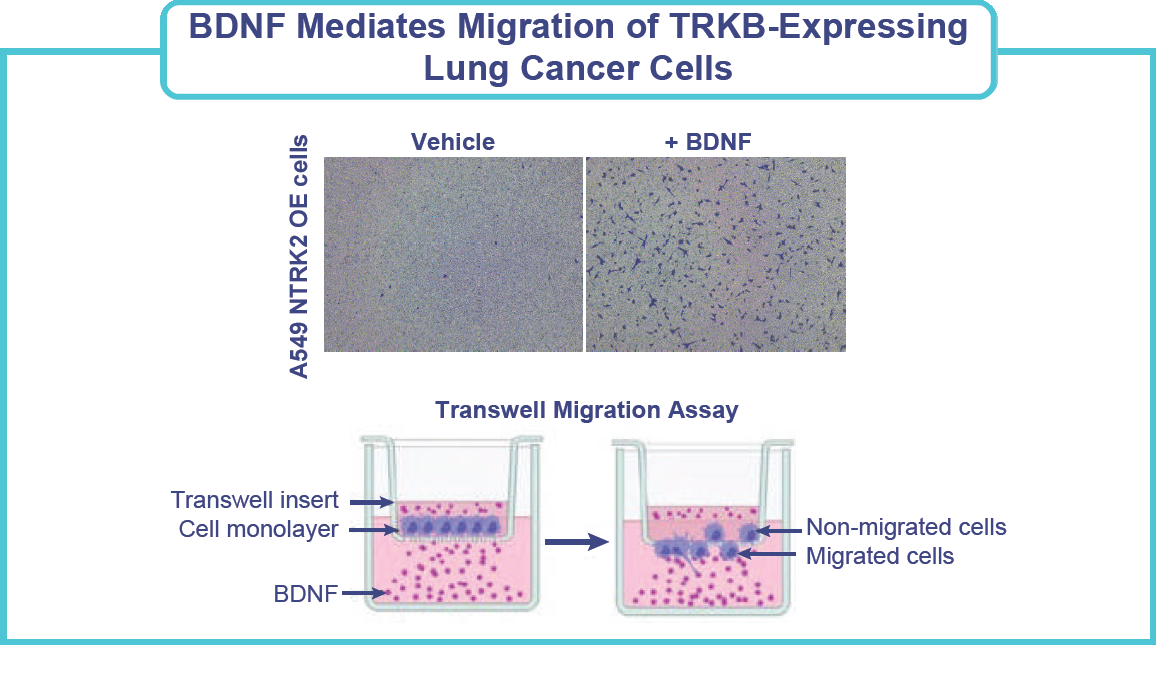
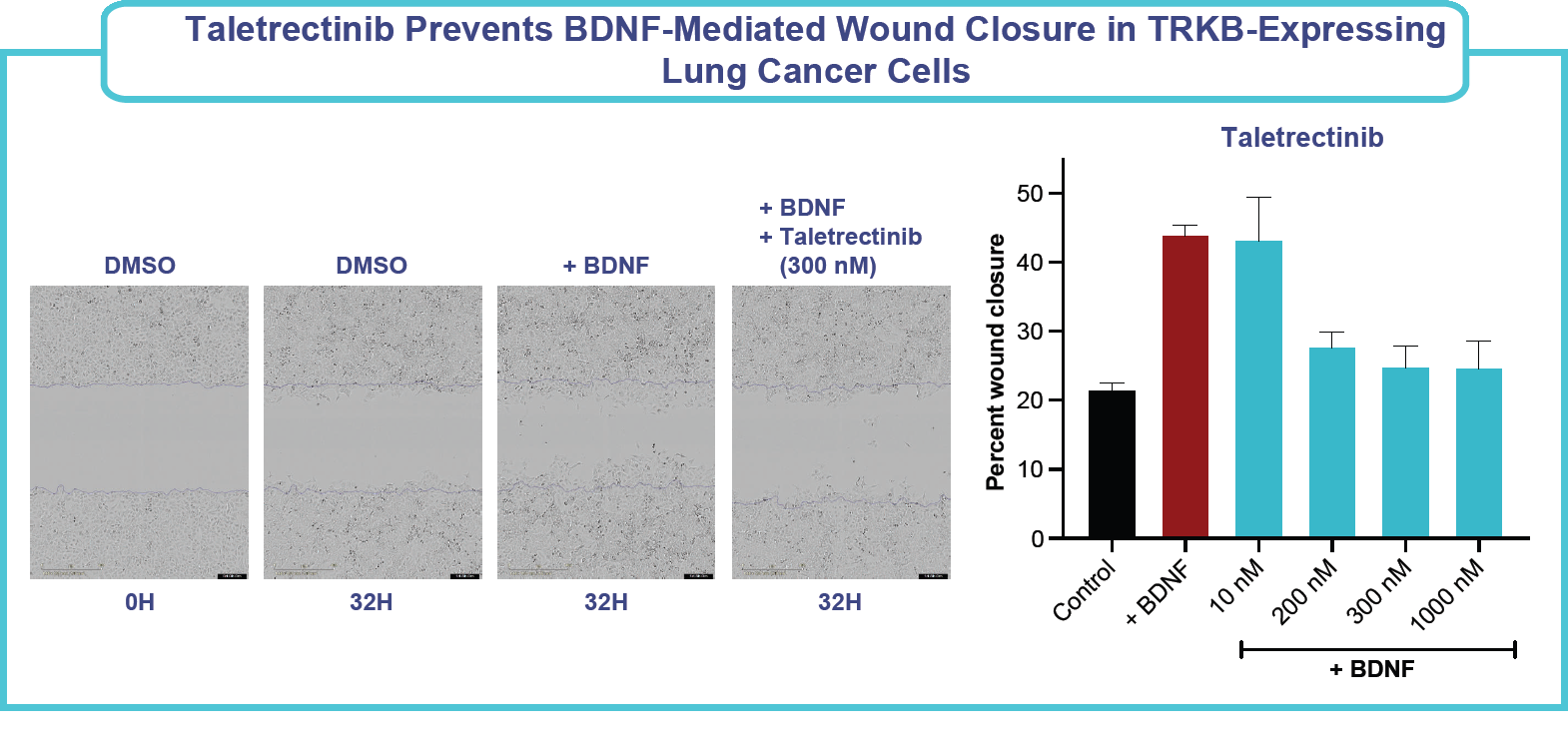
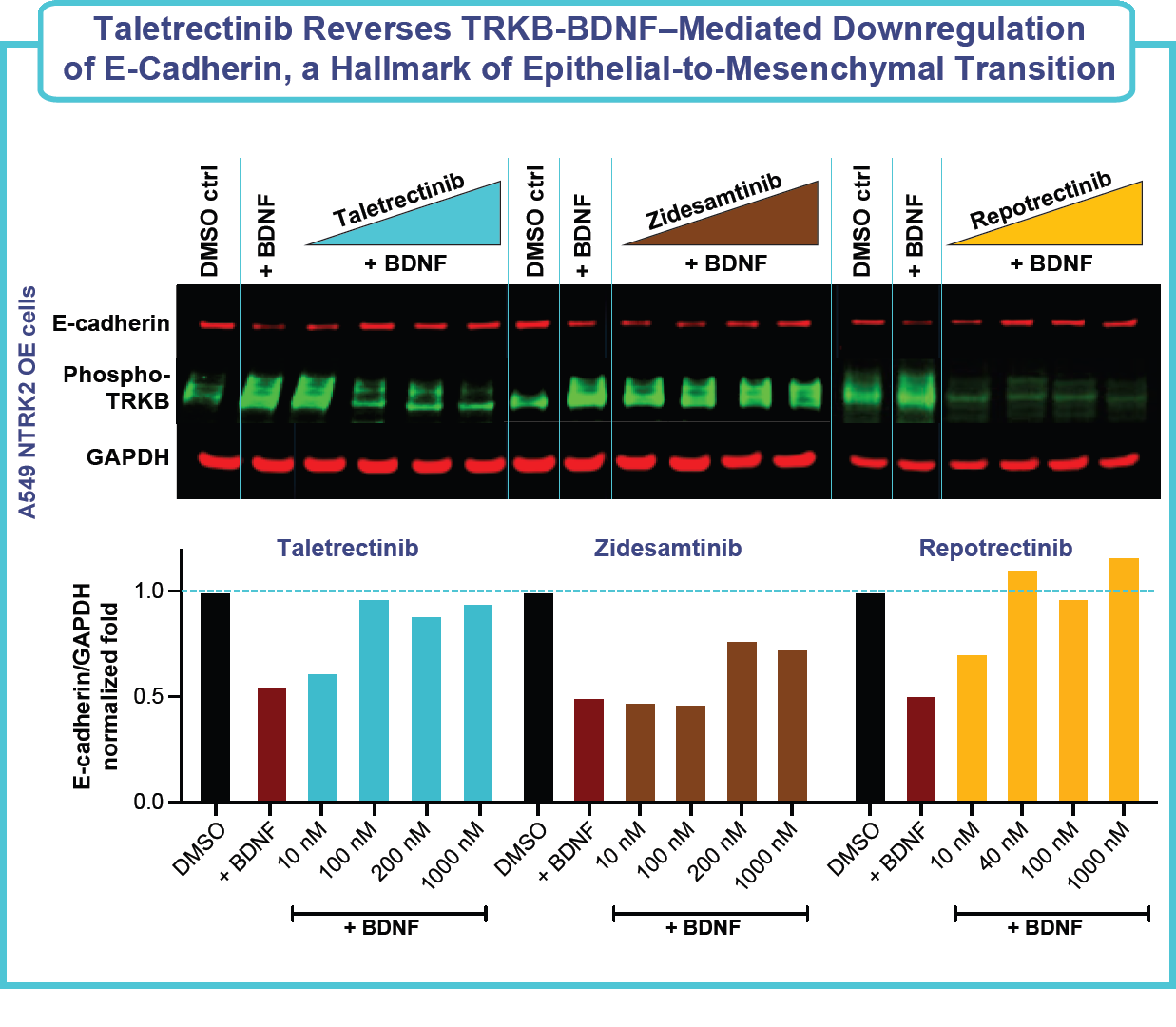
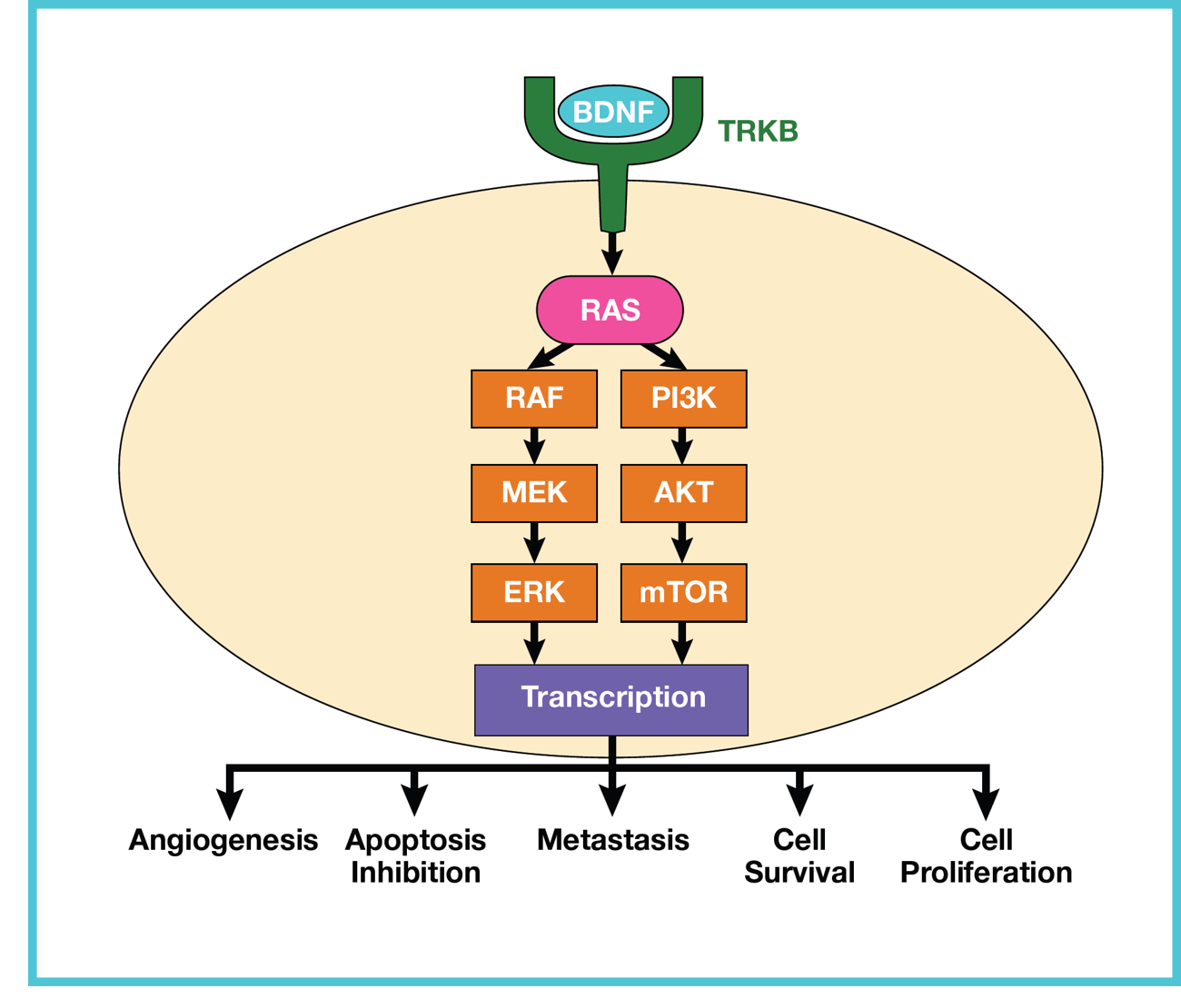
- BDNF-TRKB overexpression and signaling has been associated with increased processes involved in carcinogenesis, such as invasion, migration, epithelial-mesenchymal transition (EMT), metastasis, resistance to cell death due to loss of adhesion (anoikis), and activation of cell proliferation pathways.4
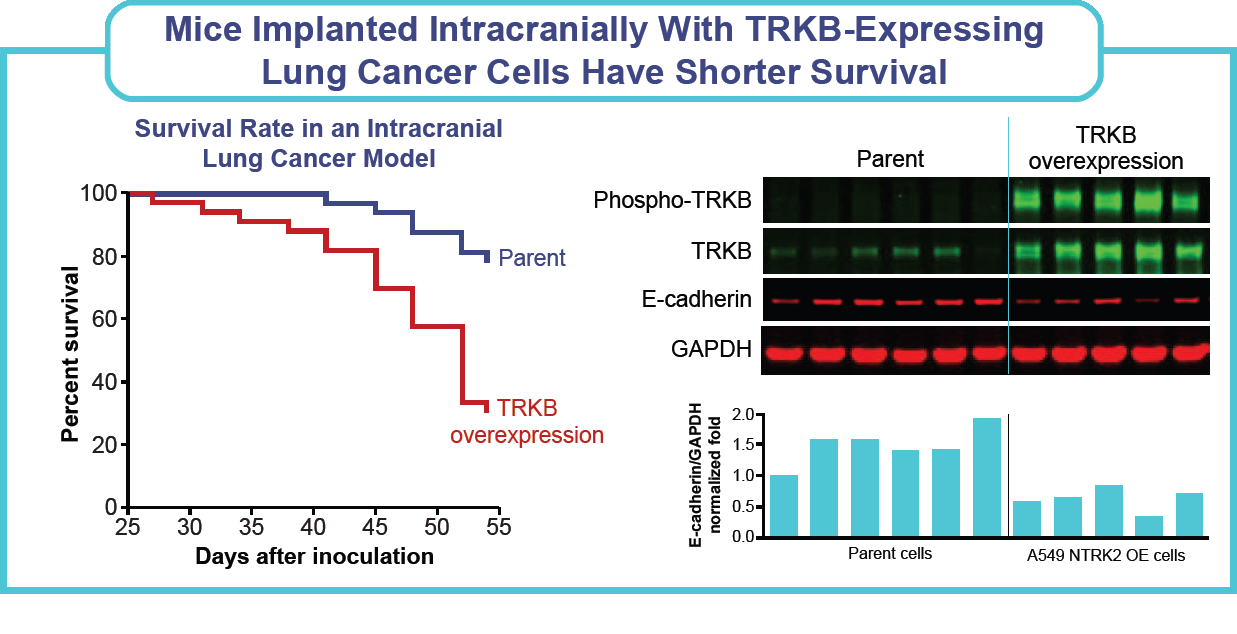
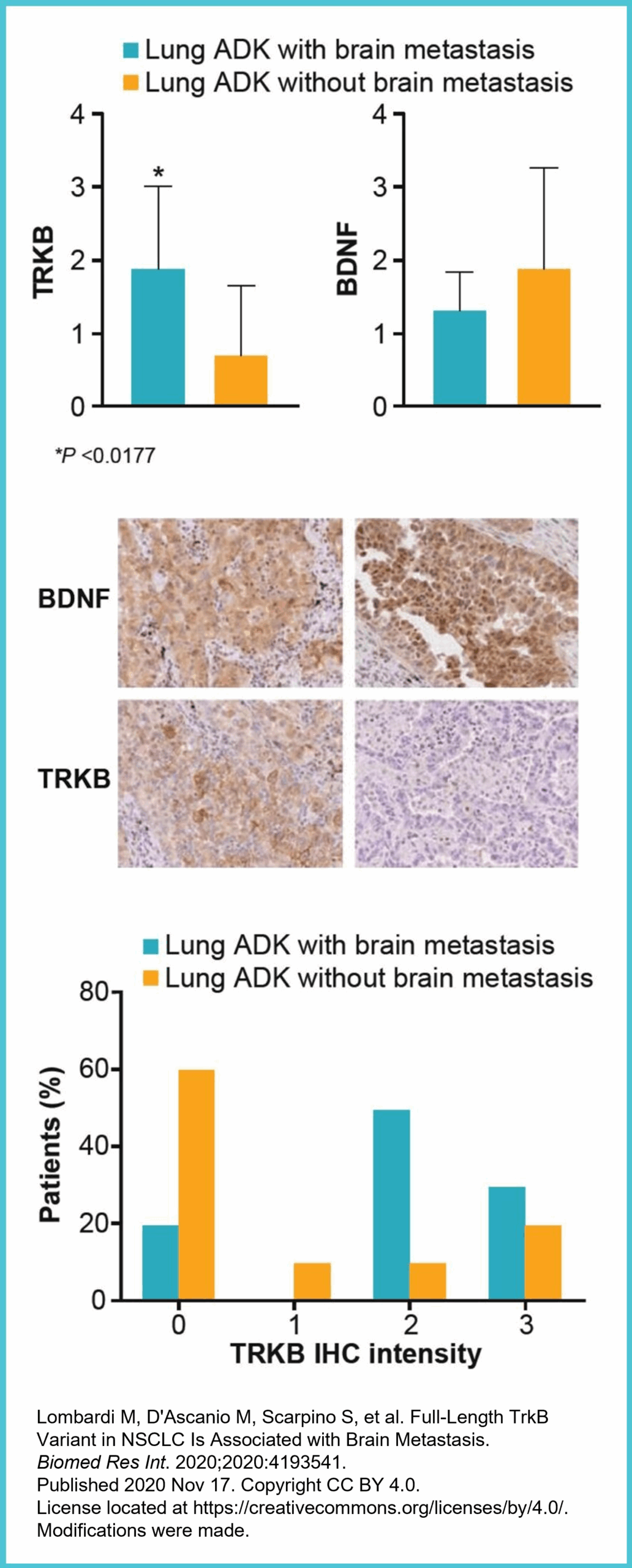
- A retrospective study showed that 80% of lung adenocarcinomas that metastasize to the CNS expressed TRKB receptor, compared with 33% without CNS metastasis.5
- There was a statistically significant increase in the TRKB protein expression in tissue samples obtained from adenocarcinomas (ADKs) of the lung obtained from lung cancer patients with brain metastasis versus patients without brain metastasis.5
- A retrospective study showed that 80% of lung adenocarcinomas that metastasize to the CNS expressed TRKB receptor, compared with 33% without CNS metastasis.5
- Recent research indicates that blocking the BDNF-TRKB signaling pathway, which regulates cancer-neuron synapses, significantly inhibits primary brain tumor progression.3,6
- BDNF-TRKB signaling regulates formation of neuron to NSCLC and breast cancer synapses which are crucial for metastatic CNS progression.3
- Given these findings, the TRKB inhibition profile of ROS1 TKIs such as taletrectinib could be clinically valuable in suppressing CNS progression.3
- ROS1 TKIs lacking TRKB inhibition may not provide the clinical value of CNS protection demonstrated in preclinical breast cancer and clinical NSCLC data.