- Taletrectinib is a next-generation, CNS-active, selective ROS1 TKI approved in the US, Japan, and China for the treatment of patients with locally advanced or metastatic ROS1+ NSCLC1–3
- Taletrectinib has demonstrated robust efficacy and a manageable safety profile in patients with advanced or metastatic ROS1+ NSCLC from two Phase 2 studies, TRUST-I (NCT04395677) and TRUST-II (NCT04919811) (Table 1)4,5
Table 1. Pooled Data From TRUST-I and TRUST-II4,5
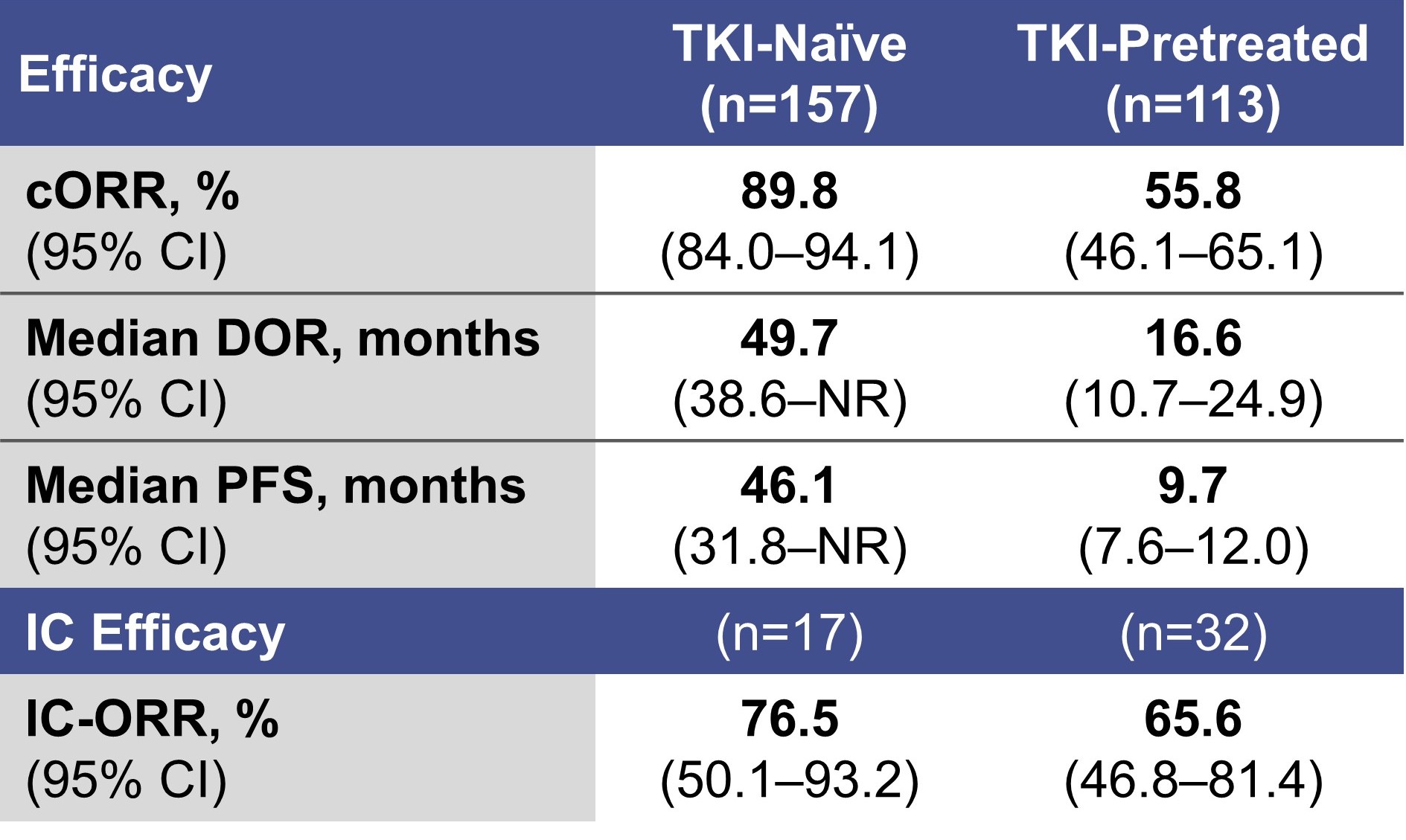
- With a median DOR of 49.7 months in TKI-naïve patients,4 it is important to understand the impact of taletrectinib on HRQoL over time
- Here we report PRO/HRQoL outcomes from TRUST-II
- At data cutoff (August 31, 2025), the PRO analysis set included 69 patients across all TRUST-II cohorts (23 TKI-naïve and 46 TKI-pretreated; Table 2)
Table 2. Baseline Characteristics (PRO Analysis Set)
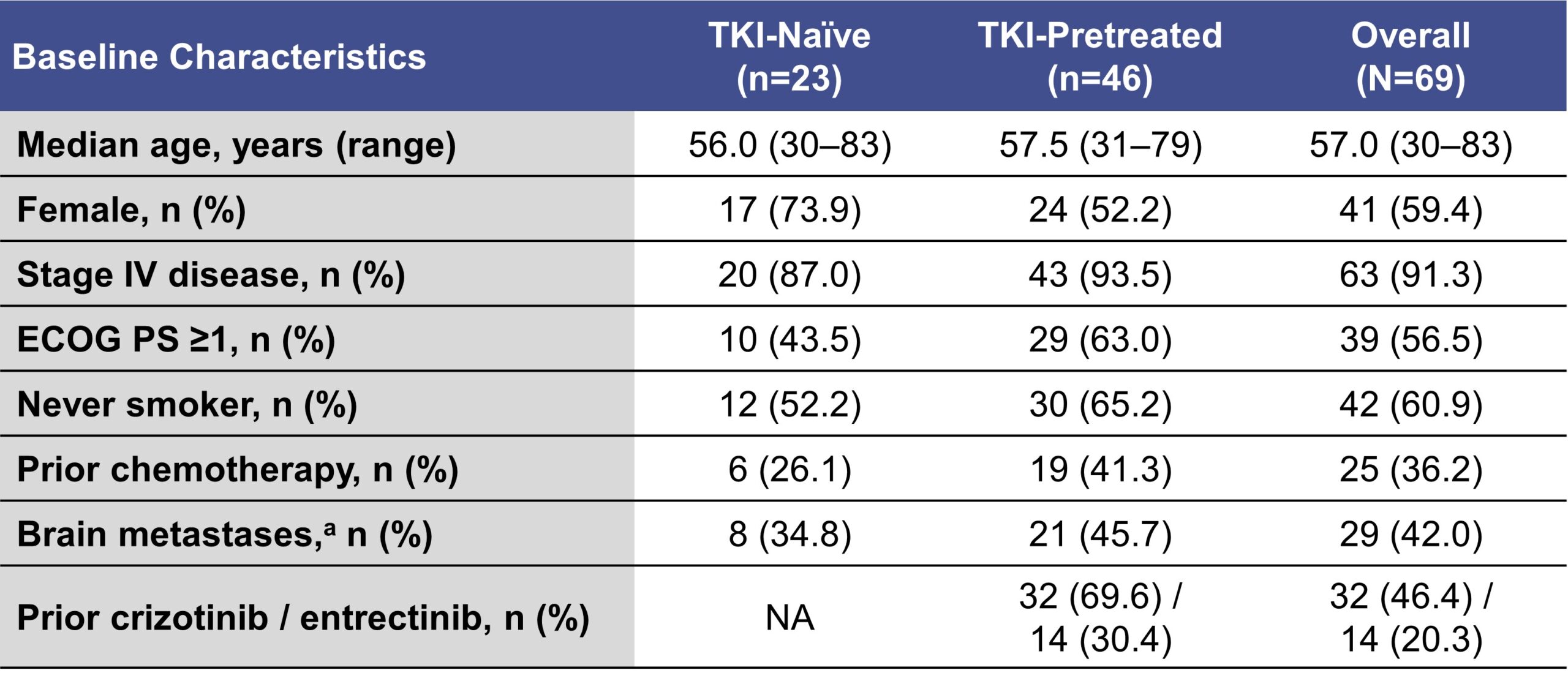
aAssessed by IRC per mRECIST v1.1.
- Mean changes from baseline improved or remained stable for most domains across both questionnaires
- Scores for GHS/QoL and cognitive function improved or remained stable over time from baseline in the overall population, as well as in TKI-naïve and TKI-pretreated subgroups (Figure 1)
- Overall, 88% of patients demonstrated improved or stable scores for GHS/QoL at the first on-treatment assessment (C2D1), including 93% of TKI-pretreated patients. The majority of scores improved or remained stable across subsequent assessment timepoints in TKI-naïve and TKI-pretreated subgroups (Figure 2)
- Mean cognitive function score improved or remained stable throughout treatment, with the majority (63–77%) of patients showing improvement or stability and only 9–23% of patients showing worsening at various assessments
Figure 1. QLQ-C30: Change From Baseline in GHS/QoL and Cognitive Function
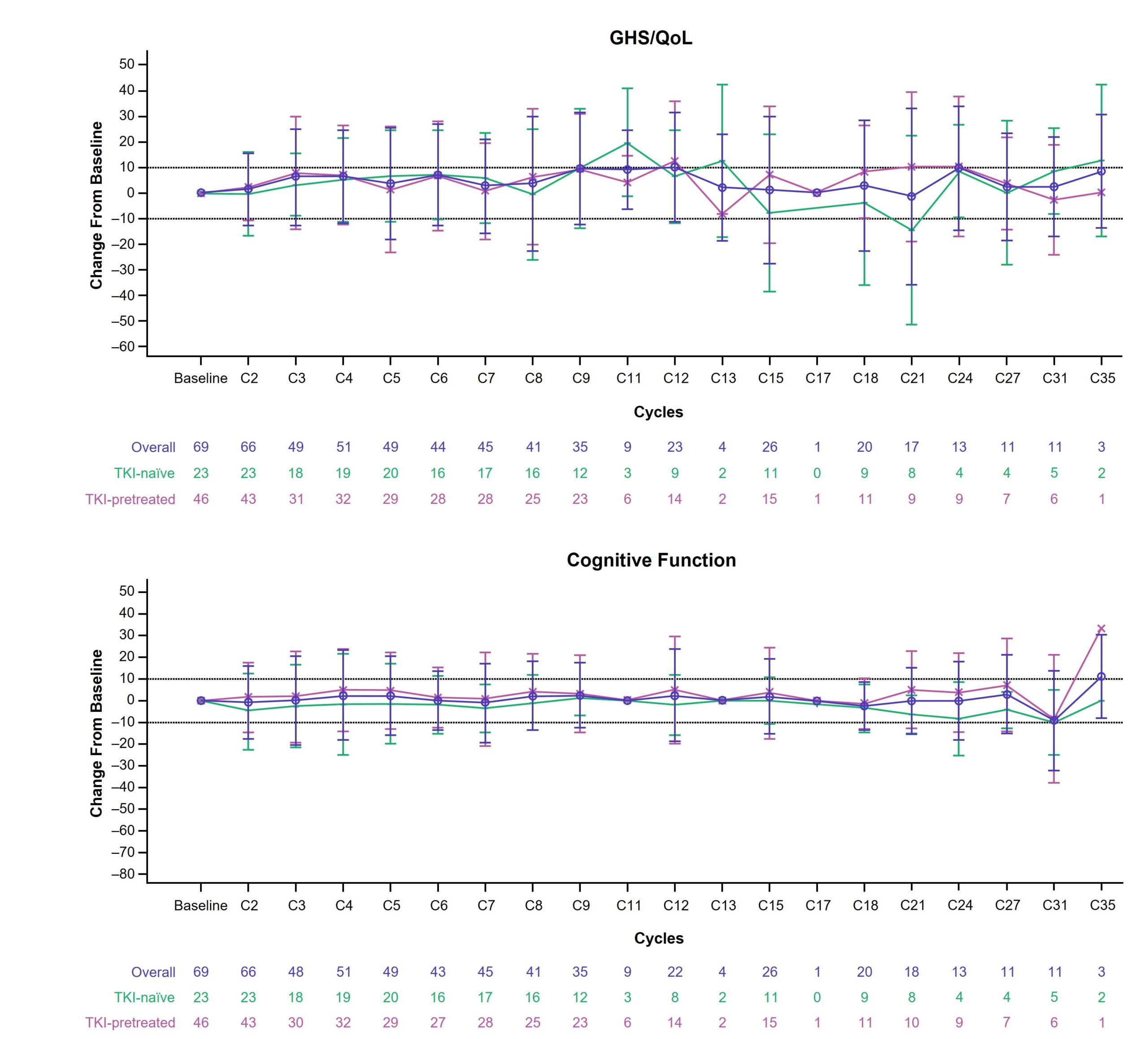
Figure 2. QLQ-C30: GHS/QoL Responder Analysis by Visita
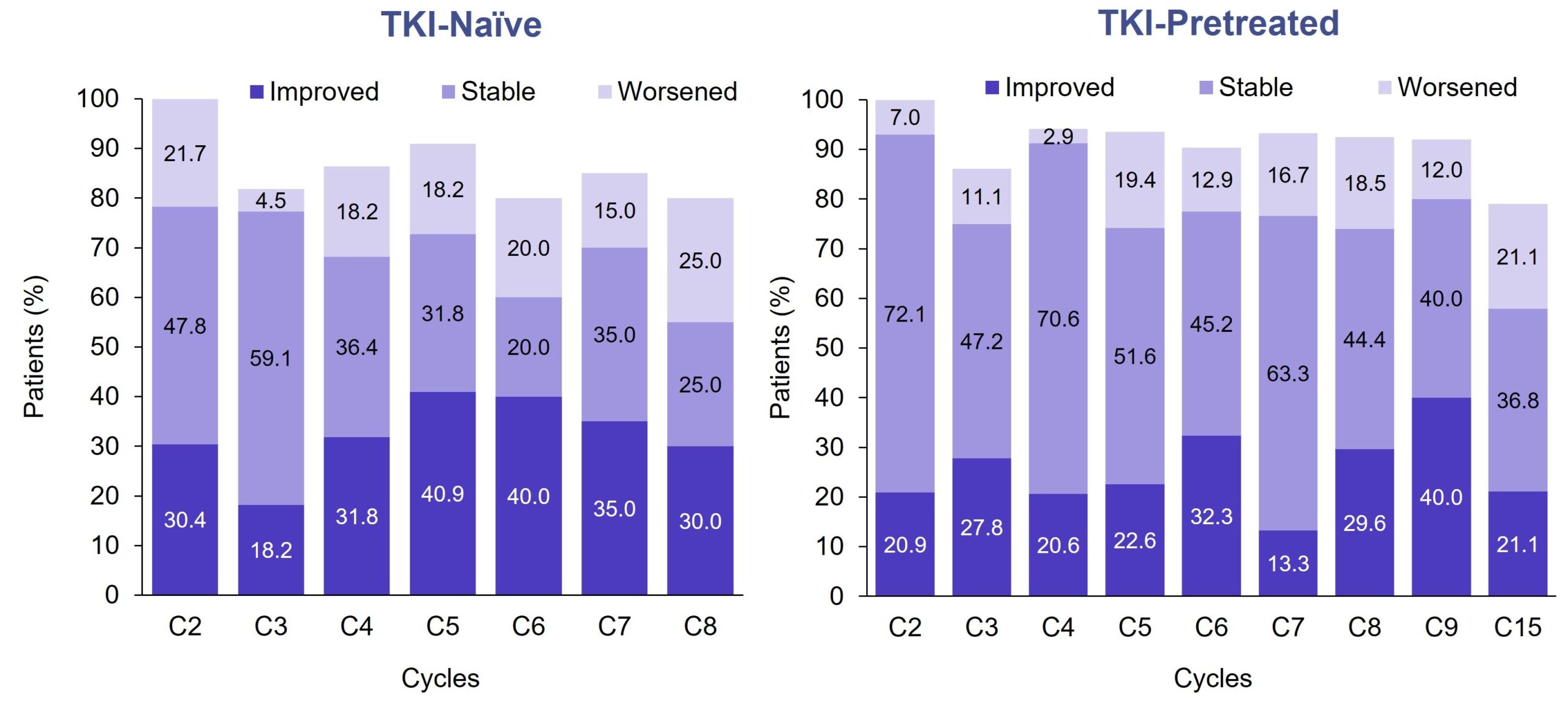
aData reported only for visits with >70% completion rates.
- At the first assessment (C2D1), 84–96% of patients demonstrated improved or stable scores for coughing and dyspnea in both TKI-naïve and TKI-pretreated patients, with no worsening of coughing observed in TKI-naïve patients (Figure 3)
Figure 3. QLQ-LC13: Dyspnea and Coughing Scores at C2D1

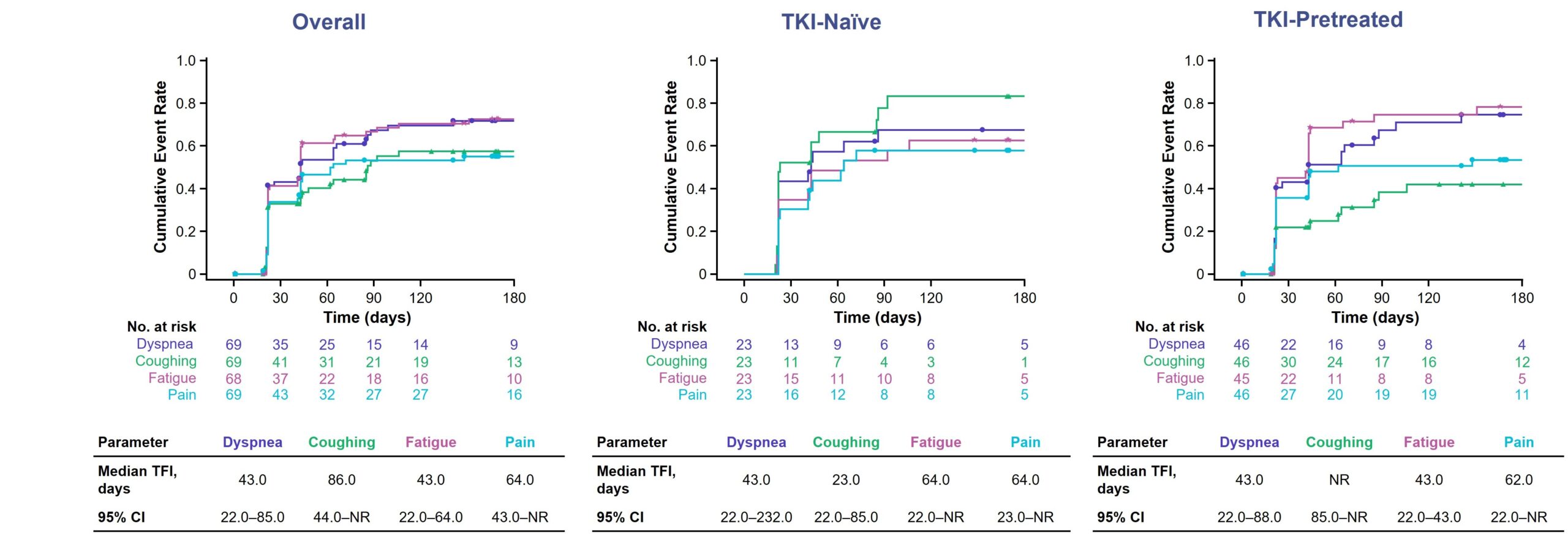
- Common disease-related symptoms, including pain and fatigue (QLQ-C30), and dyspnea and coughing (QLQ-LC13), showed consistent clinically meaningful improvement through ~8 months of treatment, with a median TFI of 1–3 months across all groups (Figure 4)
- Dyspnea and fatigue improved with a median TFI of 43 days (~6 weeks) in the overall population
- Coughing improved rapidly in TKI-naïve patients within the first treatment cycle, with a median TFI of 23 days
Figure 4. QLQ-C30 and QLQ-LC13: Cumulative Incidence of Improvement for Selected Symptom Items